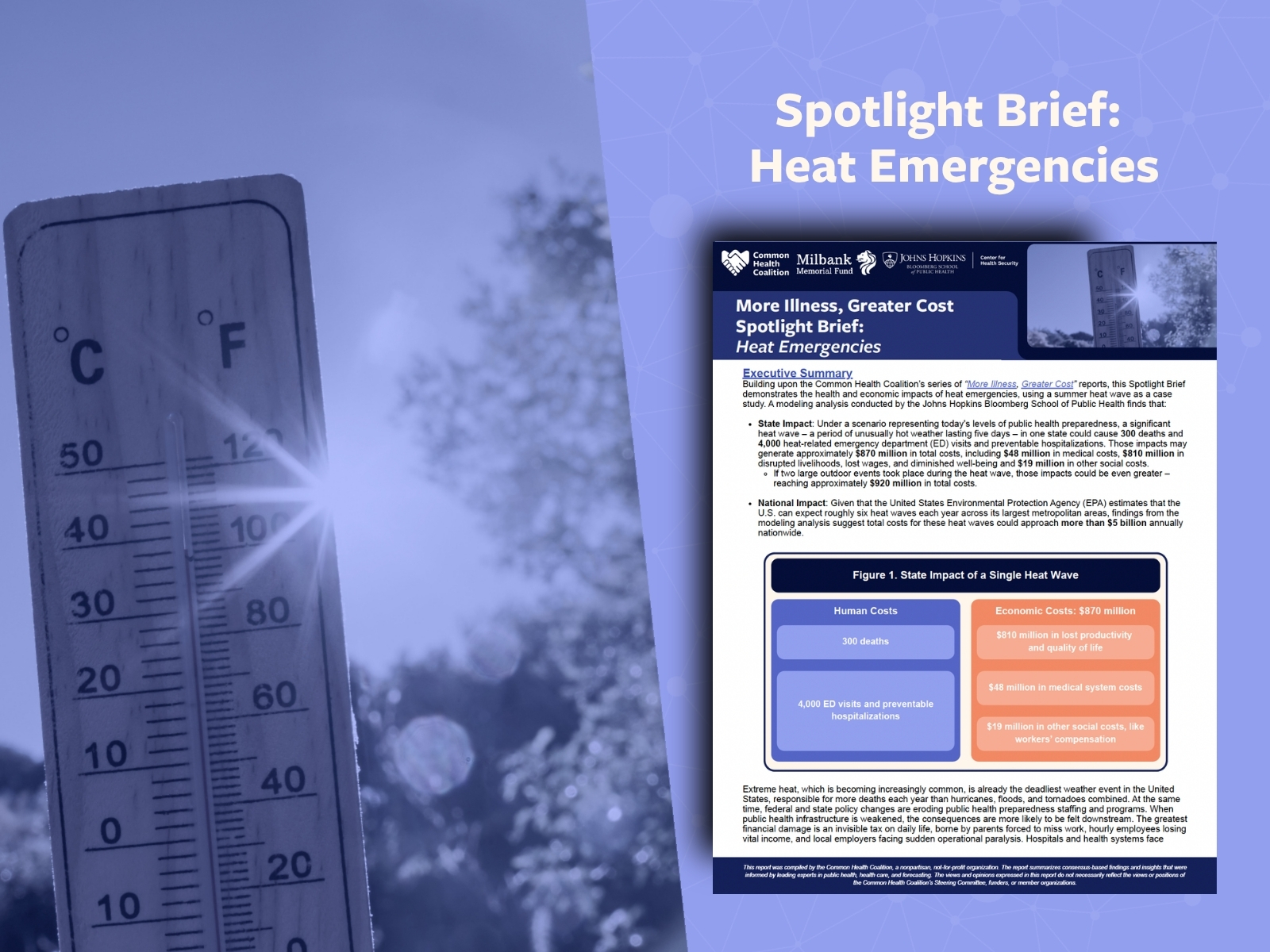
Check out the accompanying slide deck from our webinar on the health and economic impacts of extreme heat — and how to improve preparedness for heat emergencies.
Watch our webinar on the health and economic impacts of extreme heat — and how to improve preparedness for heat emergencies. Hear from researchers, public health, and health care experts as they highlight the findings of our new modeling report, 'More Illness, Greater Cost Spotlight Brief: Heat Emergencies,' and what they mean for communities across the country.
These tables outline the potential outcomes, risks, and actions associated with the ongoing changes of vaccine policy in the United States. Included are potential implications to help anticipate and navigate any public confusion that may follow.
This tracker covers anticipated outcomes, risks, and actions across payers, providers, public health, and the public related to the US Preventive Services Task Force, alongside a comparative analysis of evidence review bodies that could inform preventive-services guidance.
A policy tracker exploring state legislative and executive actions around vaccine access, including an overview of current vaccine infrastructure by state. This tracker is updated regularly.
This model bill creates a state-controlled framework that activates when federal programs do not apply. It protects providers following medical guidelines while ensuring fair compensation for rare injuries, while limiting state financial exposure.
The Coalition's approach to economic analysis of health policies is designed to be useful in the real world. It is fast, affordable, specific, grounded in practitioner knowledge, and ends with solutions. We give health leaders the right information in time to act on urgent health issues, and build the cross-sector trust that makes action possible.
Public health challenges are growing while traditional funding streams shrink. The Coalition’s Shared Financing Approaches allow communities to pool resources, reduce risk, and align incentives to invest in sustaining vital prevention programs. Tags
A federal judge in Boston has temporarily blocked three major actions taken by HHS Secretary RFK Jr. and the CDC that changed childhood vaccine recommendations, by issuing a stay. What this means for health leaders, patients, and their families.
Showing 1-12 of 91
Compendium
Compilation of effective activities happening at the intersection of health care and public health.